Blockage of the tear drainage system often leads to troublesome watering and discharge and at times, acute infection of the lacrimal sac among patients of all age groups ranging from infants(congenital) to elderly, and can be cured by probing, intubation and surgery. Blockage can be complete or partial or at any site from the lacrimal puncta to the nasolacrimal duct.
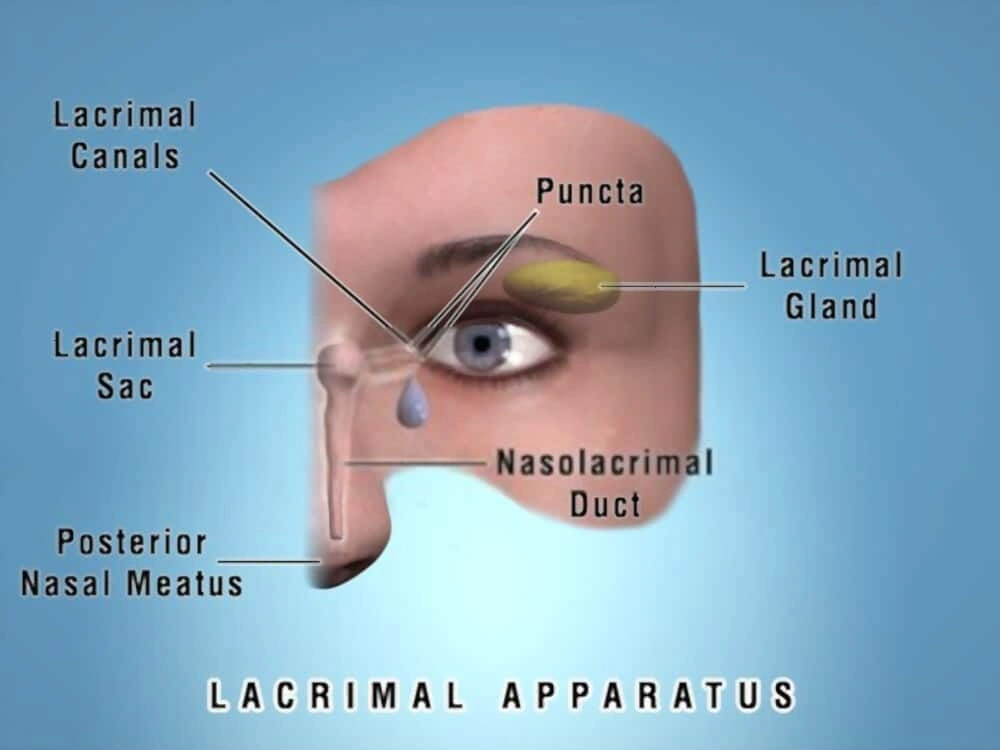
Lacrimal Apparatus
Probing
Every eye has a fine pipe leading from the eye into the nose. This is like a drain-pipe, and the tears go into the throat through this pipe. This is called the nasolacrimal duct. A child may be born with a block in the naso-lacrimal duct; this condition is called congenital dacryostenosis. The water and sticky material come out of the eye, and the child’s eyes appear to the tearing all the time. This condition is seen within a few weeks after birth.
Many of the children with congenital dacryostenosis will heal only with antibiotic drops and sac massage. The oculoplastic surgeon will show you the correct technique of sac massage for your child. If the condition has not healed by 9 to 12 months, it will probably not respond to further massage and a surgery will be required.
The first step of surgery is called probing. It is very safe, can be done as a day-care procedure (night stay in hospital not required). There is no external wound or stitches, no bandage required, and normal activities can be continued from the next day.
To see a video of the procedure, play the below video. (The clipping is of a surgical procedure, viewer discretion is advised.)
Dacryocystorhinostomy (DCR)
Each eye has a fine pipe which drains the tears from the eye. This is a nasolacrimal duct (drain-pipe of the eye). If it gets blocked, the tears and stickiness come out of the eye. The eye can be red or feel irritation. The treatment is by dacryocystorhinostomy (DCR). This is a technique by which a new passage is created from the eye into the nose, and the tears can drain out.
The best results are achieved at about one year of age. Nine out of ten babies have the problem corrected if probing is done within this time. As the child grows older, success chances decrease to about 7 or 8 out of 10.
If the watering does not improve with probing, what is the next step?
A probing can be repeated 3 months later, putting silicone intubation in to prop open the nasolacrimal duct. For children older than 3-4 years, we recommend using silicone intubation routinely at the time of probing. If this too does not resolve the watering, the next step is a bigger surgery (DCR) where a new nasolacrimal duct is constructed. But do not worry, the vast majority of children will recover only with probing.
Is it necessary to undergo DCR?
When a nasolacrimal duct is blocked, the dirt and discharge accumulate in the lacrimal sac next to the eye. There is the risk of severe eye infection if the condition is left untreated. There may be swelling, pain, and watering. If a cataract surgery is planned, a blocked nasolacrimal duct increases the risk of dangerous infection; a DCR should be done before the cataract surgery.
How is DCR performed? What are the outcomes?
DCR can be performed in two ways- externally, through a small (less than half inch) line next to the nose; endo-nasally- through the nose.
The external DCR leaves a fine mark near the eye; it has the highest success rates, more than 95 out of 100 patients have the problem completely solved after external DCR. An endo-nasal DCR is done through the nose, so there is no mark outside. The success rates are a little lower; the space inside the nose is not suitable in all patients for endonasal surgery. However, it works well in properly selected patients. Trans-canalicular Laser DCR is a very rapid procedure, with hardly any pain and swelling. However, some of the DCR done with laser may close down again.
I have had a DCR done already. The eye is still watering. Why?
As mentioned, about 5 out of 100 patients find that their DCR has closed down again. This may particularly happen in a patient who had multiple attacks of infection earlier, with a history of injury near the nose, or a patient who has frequent nasal allergies and colds. The DCR can be repeated, with addition of silicone intubation to prop the passage open. A typical oculoplastic surgeon will often see patients sent over from elsewhere after the DCR did not work; most such patients can be re-operated successfully